
A Parallel Universe of Sepsis Care
The 30cc/kg Gestapo does not operate in this hemisphere.
The care of sepsis is continually rewritten. Remember the days of sampling central venous oxygenation? Not me, thank goodness – that practice had already started to fall out of favor when I began training.
But, in its place: fluids, fluids, fluids, and more fluids. Thus enshrined in Guidelines and sepsis protocols: fluids. This blunt instrument remained questioned, but untested, until CLOVERS – and now ARISE FLUIDS.
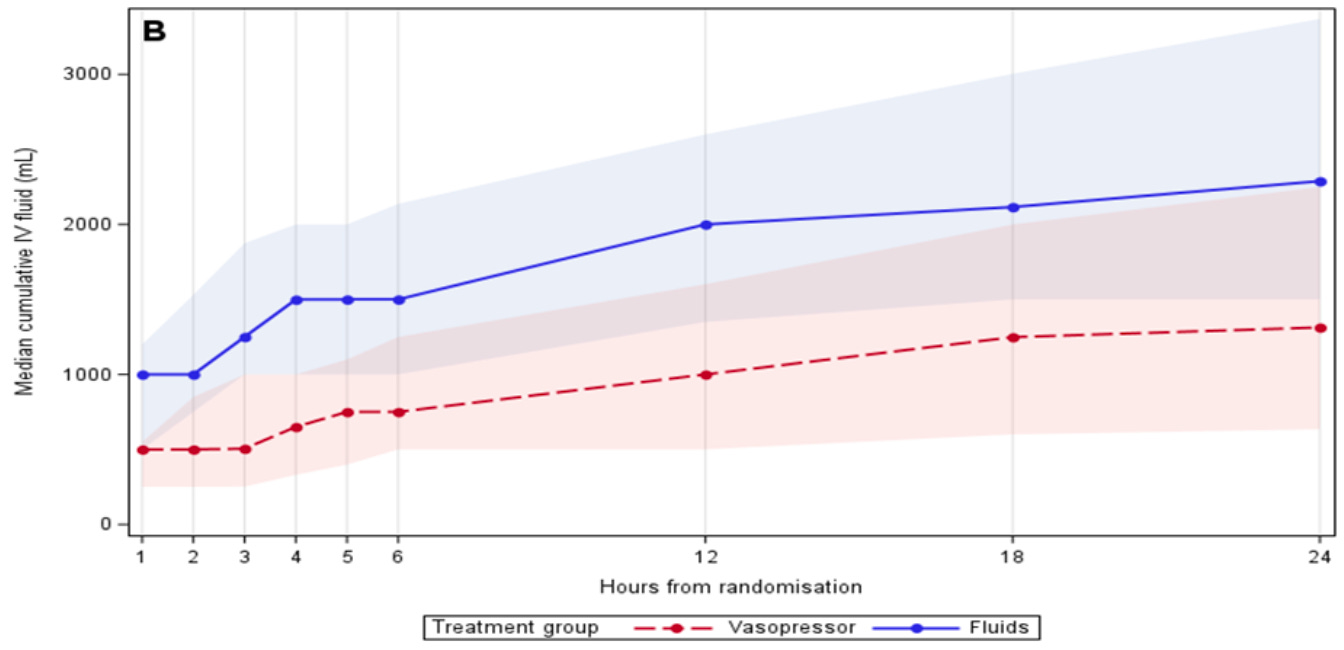
ARISE FLUIDS is an incremental step further with respect to fluid restriction. To be included, patients were enrolled in the emergency department and could not have received more than 1000mL of IVF as initial resuscitation. This allowed the total fluids curve to diverge more substantially:
And the outcomes were “similar”. The primary outcome was “days alive and out of hospital”, and this was not different between groups. There was a small point difference in 28 day mortality, but the 95% CI was 0.91 to 1.85 – imprecise enough to encompass a range of outcomes. You can see the overlapping survival curves develop a small difference early:
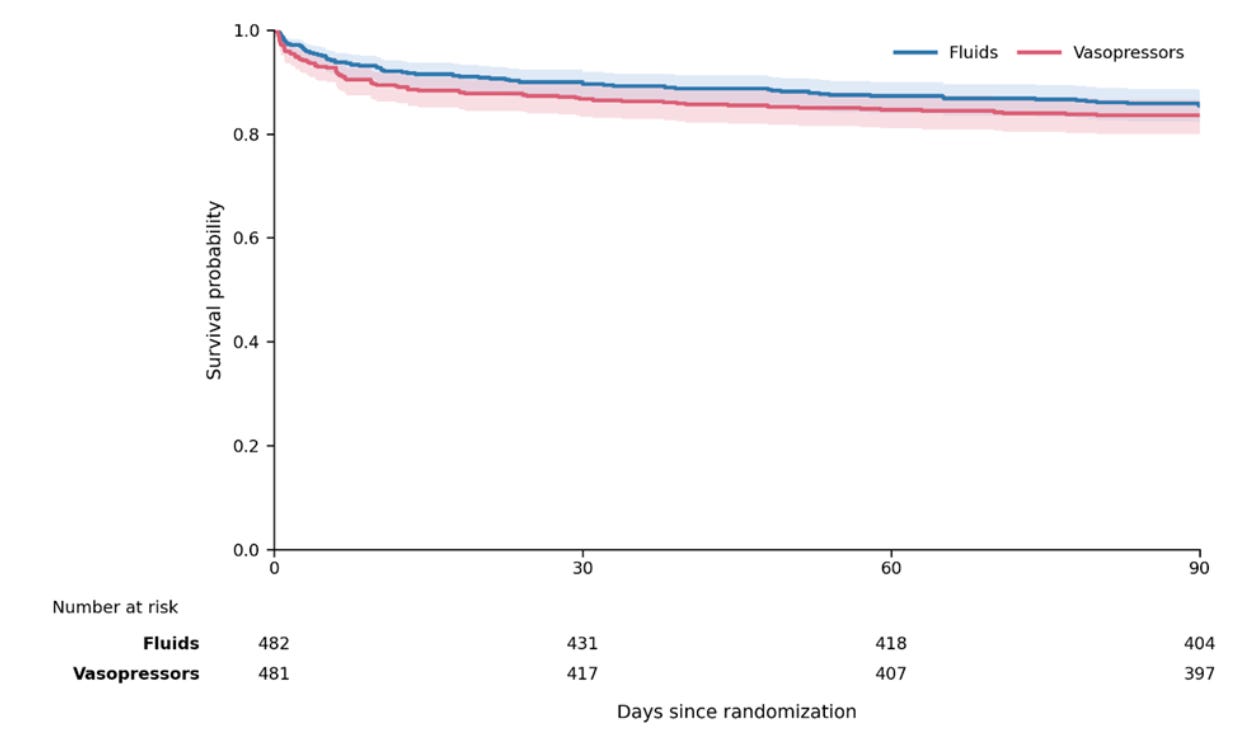
And the early – “non-significant” – difference remains durable throughout the follow-up period.
The most obvious challenge to interpreting these data from Australia and New Zealand is putting these outcomes in context next to sepsis care in other settings where typical fluid protocols far exceed even the “liberal” arm of this trial. Then, these data mostly only inform approaches to the “easy” patients who can be flexibly treated with either protocol – patients deemed “clinically unsuitable” (usually due to fluid restriction) were excluded, and these remain the types of patients for whom the question of fluids vs. vasopressors carries the greatest clinical significance.