
High-Flow Versus Standard Oxygen (in Mostly COVID)
Probably some nuance underneath to unpack.
There’s an idea (possibly related to the study sponsors, Fisher & Paykel) that "high-flow” oxygen delivery via special devices is superior to “standard” oxygen delivery via face mask. Non-invasive methods help safely reduce intubation in hypercapneic respiratory failure, but less success has been seen in other types.
This study looks at patients in French ICUs with hypoxemic respiratory failure and paO2s below 200, and if you look closely, there are differences:
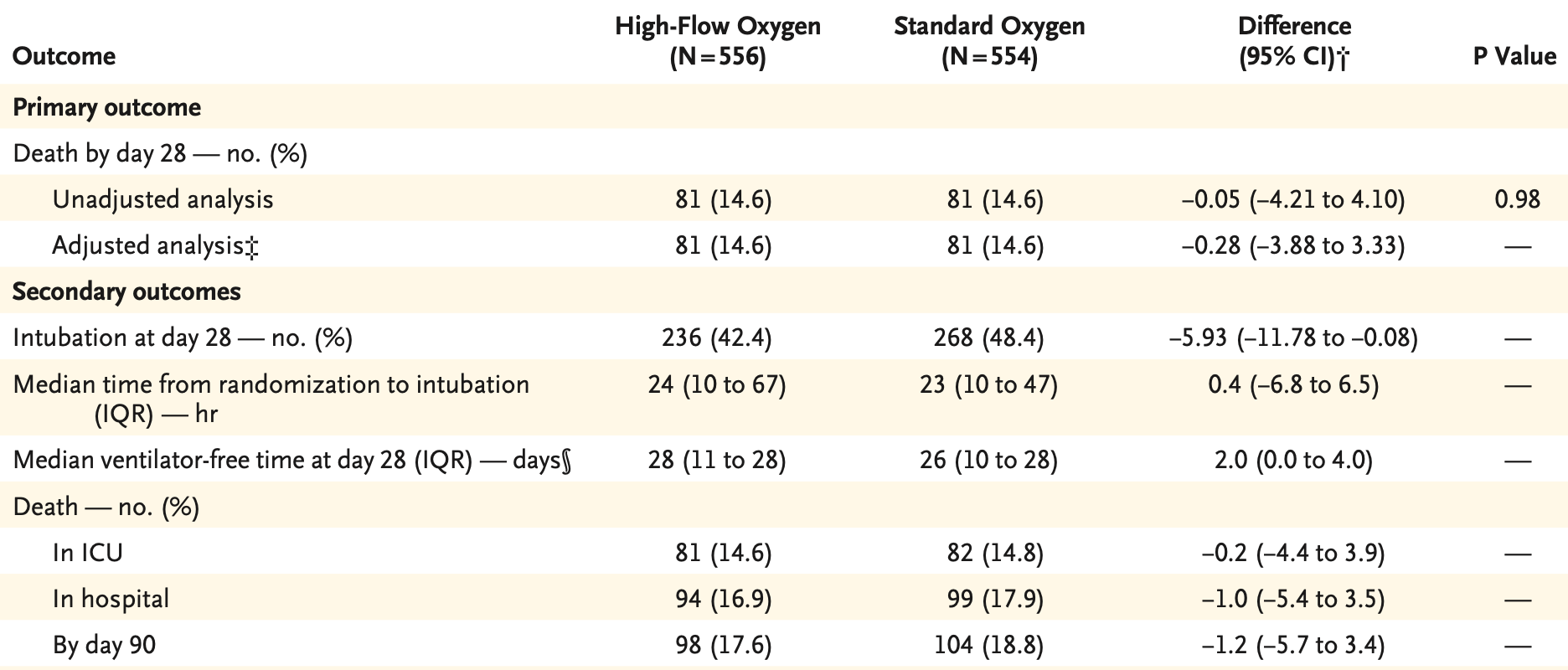
The primary patient-oriented outcome is not different. This is similar to the lack of difference identified by this same research group in their COVID-only cohort, SOHO-COVID – and not terribly surprising because about half of this cohort is also COVID-19-associated respiratory failure.
Then, SOHO-COVID saw fewer intubations in the HNFO cohort – and, consistently, again here.
It’s a bit challenging to interpret these data primarily due to the non-blinded nature of the intervention. That is to say, the presence of HNFO on a patient is likely to push clinicians to delay intubation – and it’s unclear the downstream effect on patient-oriented outcomes. There is probably some clue behind this in the subgroup analyses in the supplement:
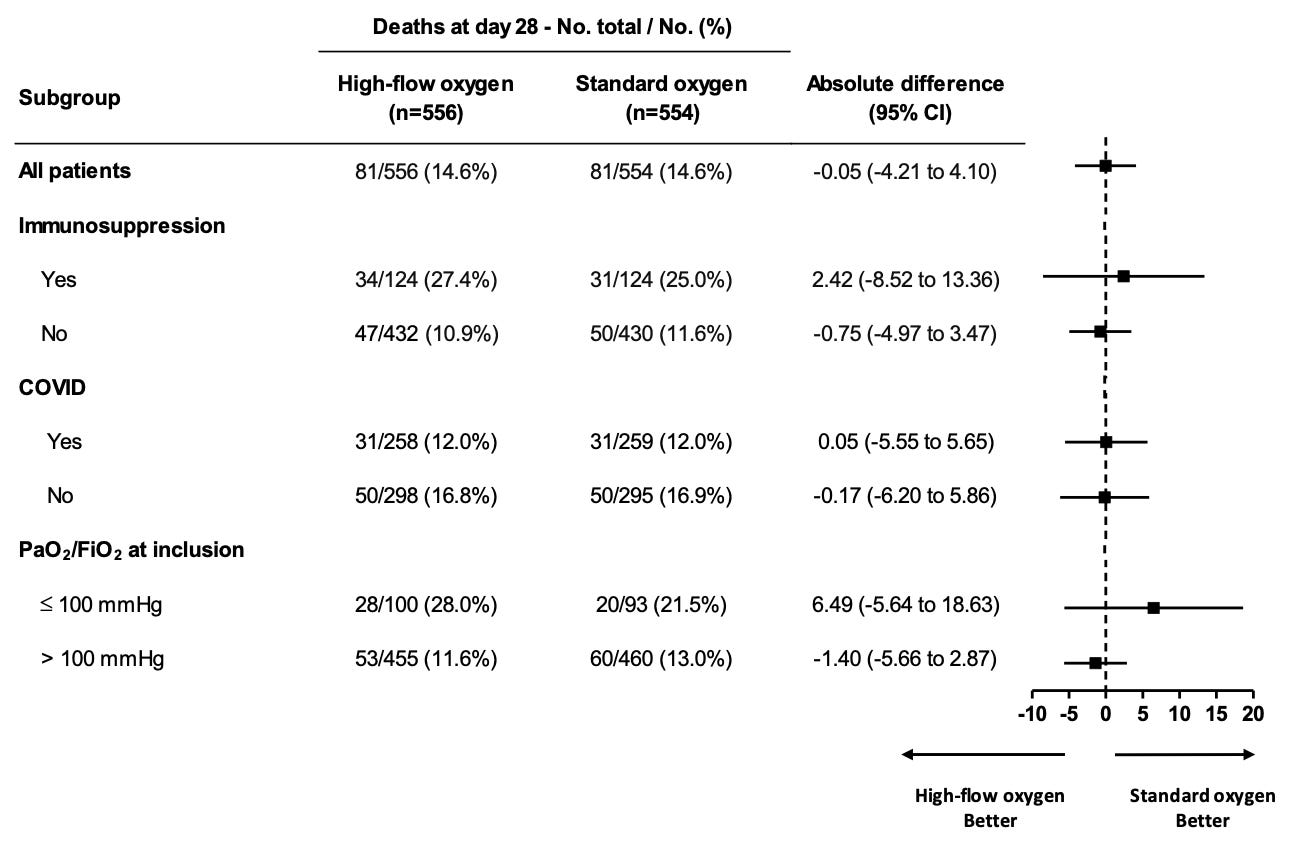
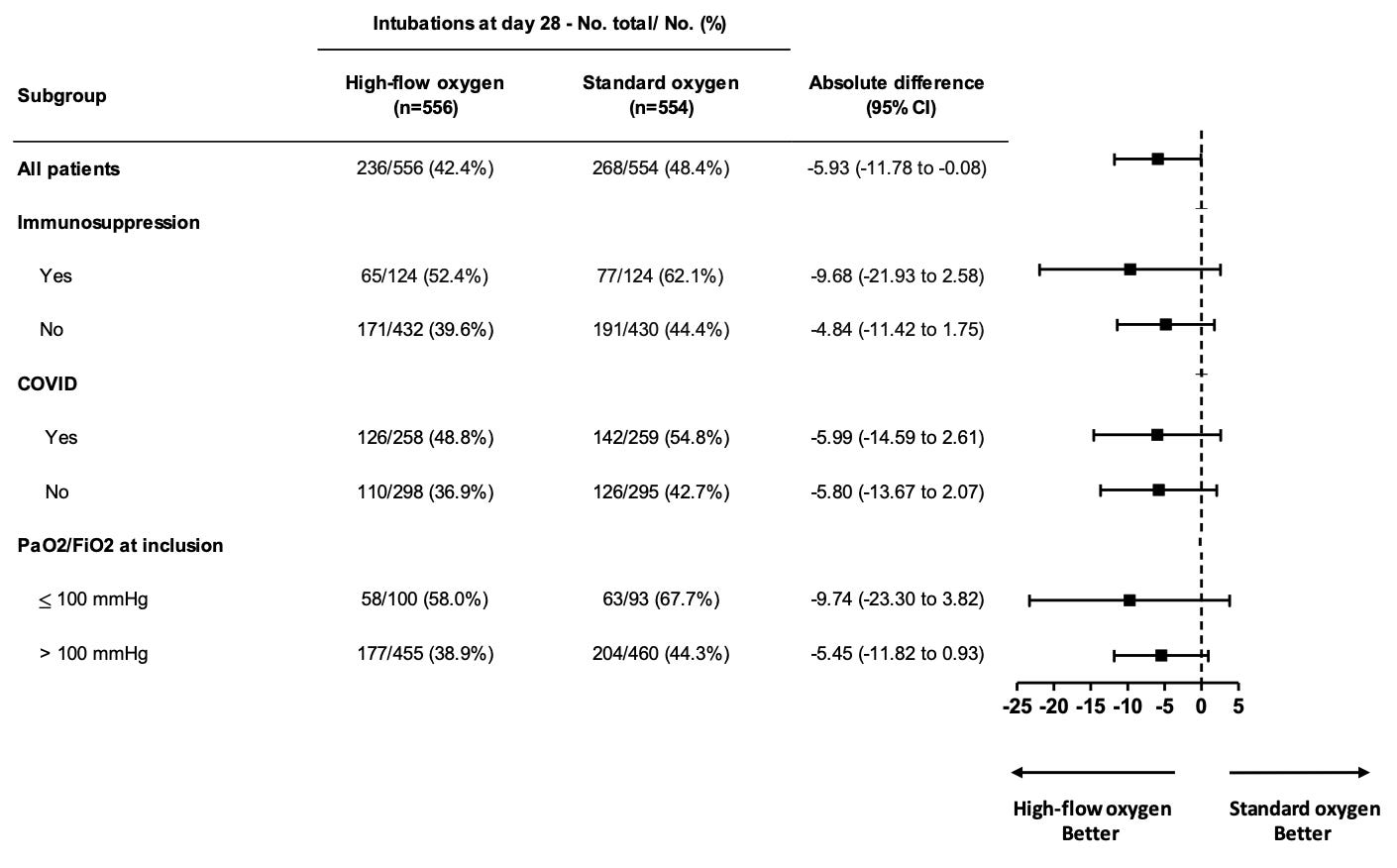
I suspect HFNO is, indeed, slightly better – but the effect of the intervention on clinician behavior needs a closer look to ensure potential harms from delayed care (intubation) are not being passed on to the patient.