
If You Look For Hepatitis C ...
You'll find hepatitis C.
The question is – how much looking for hepatitis C should you do?
In this DETECT Hep C Trial, there were two options: “nontargeted” screening, or “targeted” screening, in which screening was offered only if high-risk. In these urban hospitals in Denver, Baltimore, and Jackson, approximately 70,000 patients were randomized to each type of screening – and, unsurprisingly, more patients were offered screening in the “nontargeted” screening.
More tests offered, more tests performed – more new diagnoses of hepatitis C. As “new diagnoses of hepatitis C” was the primary outcome, the “nontargeted” screening was the “winner”:
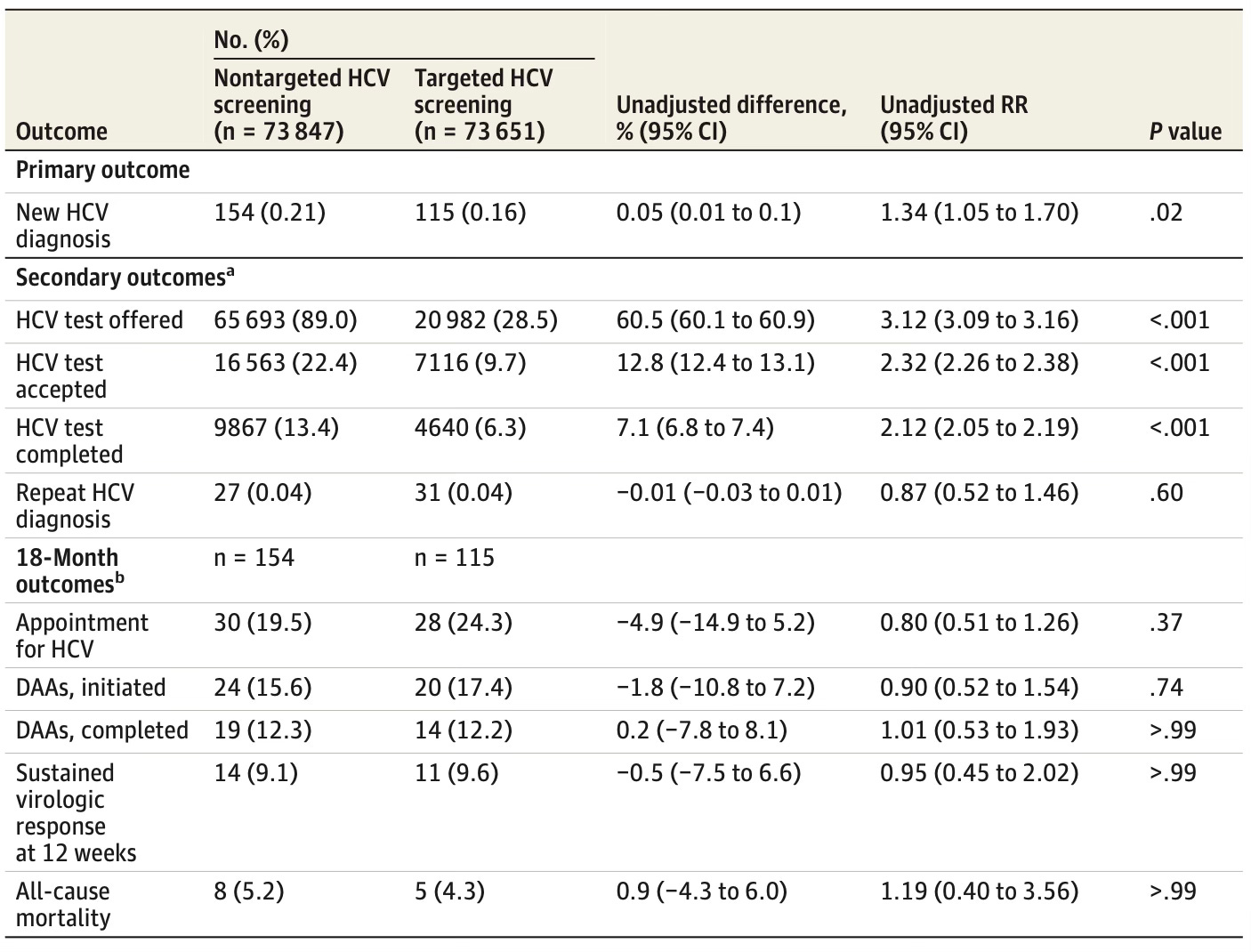
However, as you can see, of the 150,000 included in these two screening cohorts, the grand total number of patients who attended an appointment for their new diagnosis of HCV was: 58. Of these, less than half – 25 – demonstrated virologic response to prescribed antiviral treatment at 12 weeks.
The secondary outcomes don’t fully capture any long-term patient-oriented outcomes, nor a public health value stemming from the initial diagnosis – but there’s clearly a ton of work left to close the gap between identification and cure. There’s also no discussion of cost-effectiveness, though, sadly, I suspect that aspect is likely moot in this current U.S. health system funding climate.