
Is The Thrombolysis in Stroke Window Widening?
Just showing "time" is anachronistic and "tissue" has always been the key.
Ever since alteplase for stroke was approved, folks have been trying to figure out how to give more of it. This is unsurprising, considering the extent to which Genentech et al were involved in the design and conduct of the initial stroke trials.
The HOPE trial follows in the steps of WAKE-UP, TIMELESS, and TRACE-3, other trials attempting to go beyond the current 4.5 hour thrombolysis boundary by incorporating advanced imaging, similar to that seen in the endovascular intervention trials.
And, it works:
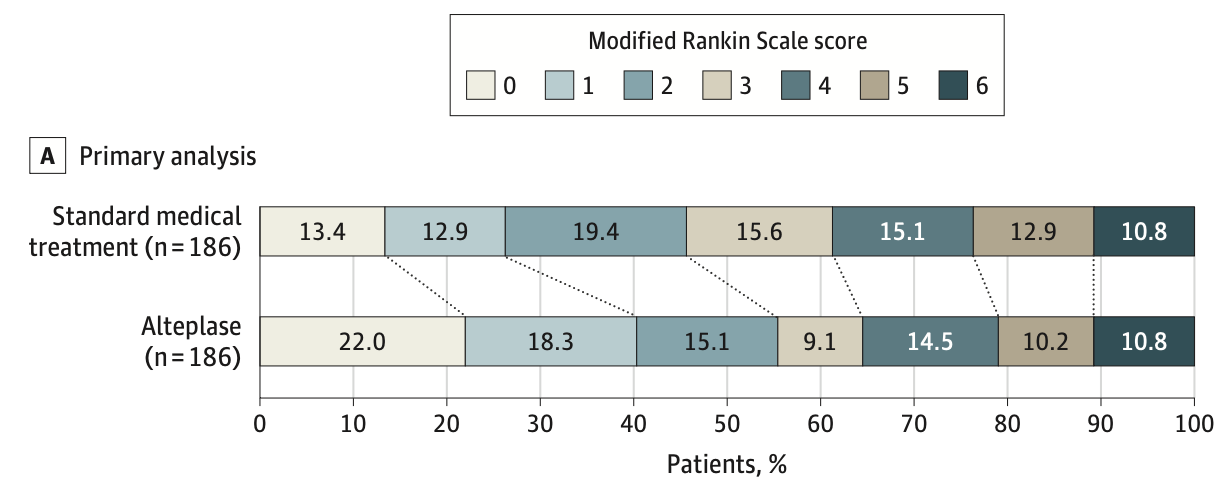
This follows what has always been a very simple A + B = C equation for stroke: if you have salvageable brain tissue (A) and a way to open the occluded vessel (B), you get better outcomes (C). If you miss out on A or B, you don’t reliably get C.
The long-standing issue with stroke treatment had been B – when alteplase was first being pushed around, it was well-known it didn’t open up many (most) large vessel occlusions. This inadequate performance for alteplase was downplayed until it became mooted by improvements in endovascular intervention.
Now, with improved imaging modalities to guide stroke care, there is more opportunity to examine A. There are clearly many strokes with small ischemic cores (folks in this trial were only about ~12mL) and large “penumbra” (about 50 mL in this trial) even outside the old, artificial time windows established prior to the availability of perfusion imaging. The flip side few are talking about, however, is that some strokes within the time windows will not have salvageable tissue – but our rush to give (sell) all-comers alteplase conveniently ignores that fact.
I, for one, applaud the replacement of time-based criteria with tissue-based criteria – as long as it applies, in reciprocal fashion, to those presenting within 4.5 hours of stroke onset, as well.