
It's the Etomidate vs. Ketamine Showdown
Because rocuronium vs. succinylcholine is settled.
Etomidate suppresses the adrenal axis. Ketamine is a vasodilator and negative inotrope. In critically ill patients undergoing tracheal intubation, which induction agent will win?
Which would you want for yourself?

Are there other clinical features that matter?
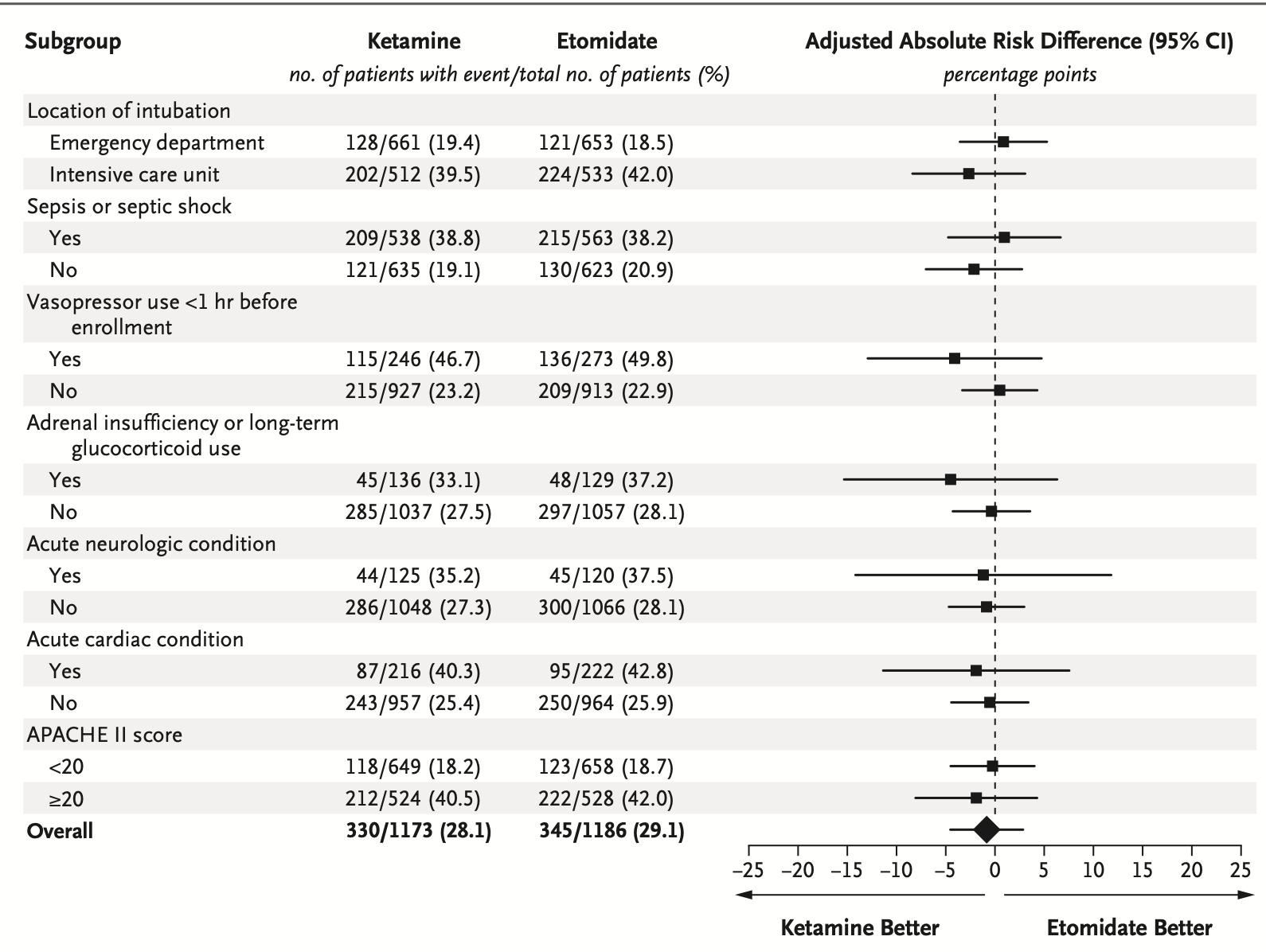
So – not really much in the way of reliable differences. Additionally, there’s a sensitivity analysis for death in any location by day 28, not just in-hospital death, and there was literally no difference on that outcome.
So, ketamine vs. etomidate – whichever agent you feel appropriate for the situation is likely as good a choice as the other.
As hypothetical aside, it’s always an interesting question: “what’s the minimal clinically-important difference?” for an outcome. The observed difference in the primary outcome here is 1.0% – meaning the net clinical effect (95% CIs notwithstanding) is that one extra person will suffer in-hospital death per every 100 intubated with etomidate instead of ketamine. If everyone switched to ketamine where feasible, there would be hundreds, if not thousands, of additional survivors each year. Is that “important”?
In the Supplemental Appendix, the authors make their case – and land on a 6% difference. How did they choose 6%? Well, they looked at what previous trials did, in context with estimates of ARR required to make a group of surveyed intensivists change practice. So – MCID is not about the patients and their outcomes, it’s actually about the difference required to make clinicians change practice. It’s also a happy coincidence a larger MCID gives you a smaller sample size – if 1% were the expected MCID, attaining a 95% CI that didn’t cross unity would require a much larger sample than the 2,365 randomized here.
In this case, the 1.0% difference is just as likely to be statistical noise as not – and the 28-day “any location” mortality cinches it. I’d happily argue even such as a small, if reliable, difference in mortality would be enough to tilt my practice, but the MCID discussion here is likely moot.