
Minor Updates For Minor Stroke
Minor stroke is all in the eye of the beholder.
If the general stroke thrombolysis debate remains a valid point of contention, then, even more absurd becomes the idea of thrombolysis in minor stroke. Yet, despite a gross paucity of evidence, here we are.
This clinical review breaks down the evidence and distills it down into recommendations encapsulated in this information graphic:
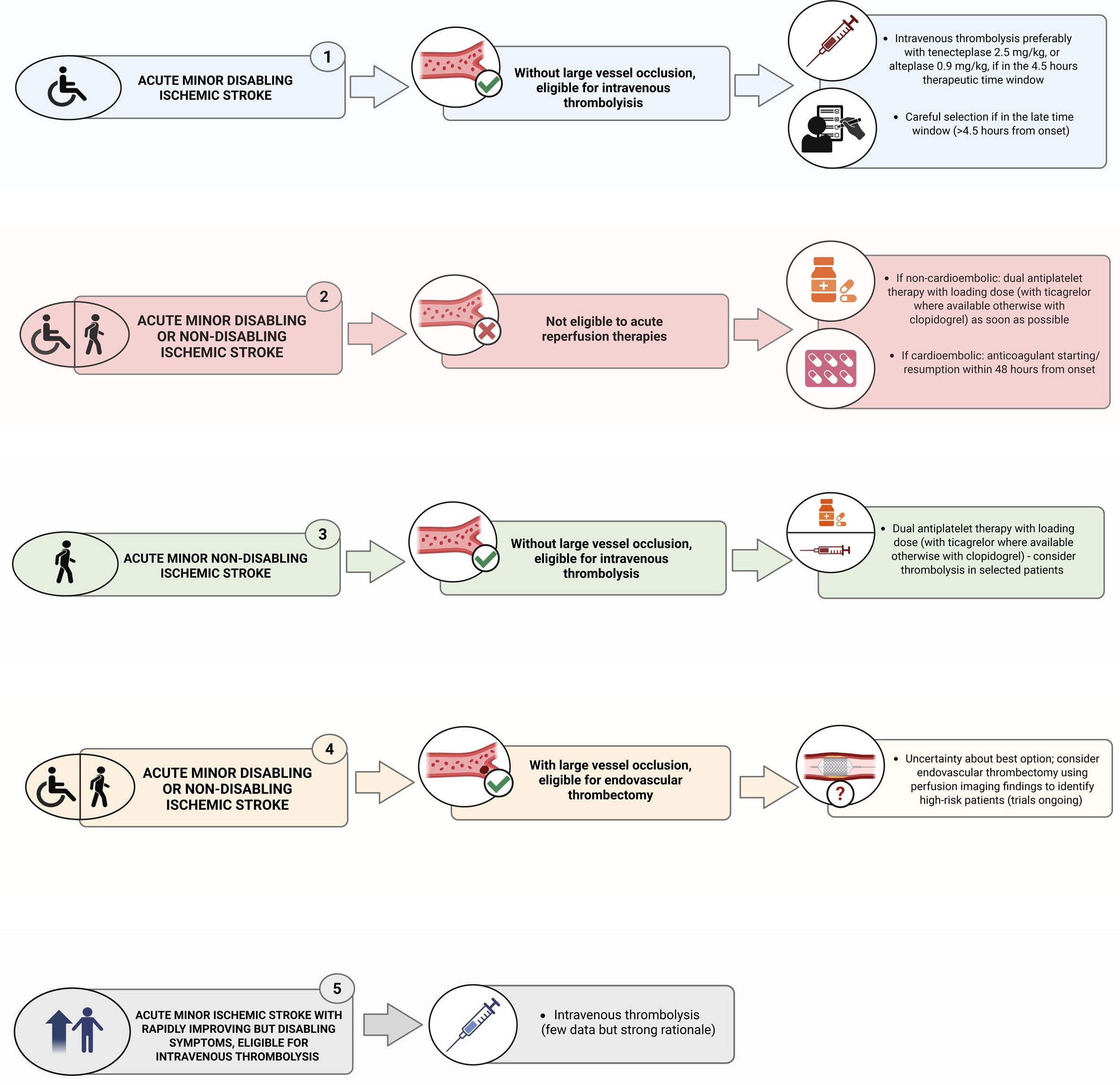
As you can see, the needle shows up quite frequently – and these authors yet again do the (lack of) evidence a disservice. Every RCT specifically enrolling patients with minor stroke has come up with harms resulting from IVT: PRISMS, ARAMIS, PUMICE, and TEMPO-2. The “out” neurologists have in these situations is that these primarily enrolled patients with “non-disabling stroke” – and recommendations for IVT involve “disabling” stroke. Instead, they point to the Emberson individual-patient meta-analysis and the 666 patients with NIHSS 0-4 included – and an aOR of [1.07 - 2.06] for better outcome with IVT in this cohort.
However, studies parroting the Emberson aOR persistently decline to note 400 patients out of this 666 cohort came from IST-3, and the NIHSS 0-5 results actually favored the control group in that trial [0.52 - 1.38]. Likewise, in the 58 NIHSS ≤ 5 patients in the NINDS trials, there was no difference in outcome between IVT and control [0.20 - 3.63]. Any apparent favoring of IVT must therefore come from skewed, small cohorts in the remaining included trials. There’s no reasonable basis for drawing a strong conclusion IVT is appropriate even in minor, disabling stroke.
Finally, the definition of “disabling” stroke completely hamstrung by its lack of definition – a subjective, individualized assessment of the degree of functional impairment suffered by a patient with minor stroke. Stroke is heterogeneous enough with anatomy, occlusion type, and collateral circulation, without tossing in a further subjective component to treatment decisions. Then, given the medicolegal environment in the U.S., there is virtually no incentive not to treat given the lack of certainty over patient-centered values or potential for downstream liability. In a word: chaos.
These authors do a disservice by failing to mention equipoise absolutely remains for minor stroke with disabling symptoms – other than to note a structured definition of “disability” would greatly help clarify treatment decisions.
<END RANT>
I'm interetsed to find out if tnk works at all in lacunar strokes or (small-ish) strokes that have no salvageable penumbra, at all, regardless of the severity. (it's 2026, MRI exists now)
You can have a tiny <1 mm artery occlude and get a disabling lacunar stroke. how is tnk going to lyse that tiny vessel open, it's all calcium, atherosclerosis, lipohyalinosis in there.
And conversely, perhaps the reason tnk fails with minor stroke is precisely because most minor strokes are little, there's nothing to lyse..
PS
check out the tenCRAOS trial in the nejm, if you haven't already.