
Procalcitonin Saves Lives
Just don't ask us how.
Many folks find procalcitonin testing to be nannying and unhelpful, foisted upon them by sepsis overlords. It is, after all, little more than an expensive C-reactive protein – another non-specific marker of inflammatory response without adequate sensitivity to be relied upon to exclude all serious infections.
But, in a quite large, pragmatic, randomized, controlled trial – the PRONTO trial in the U.K. – it saved lives:
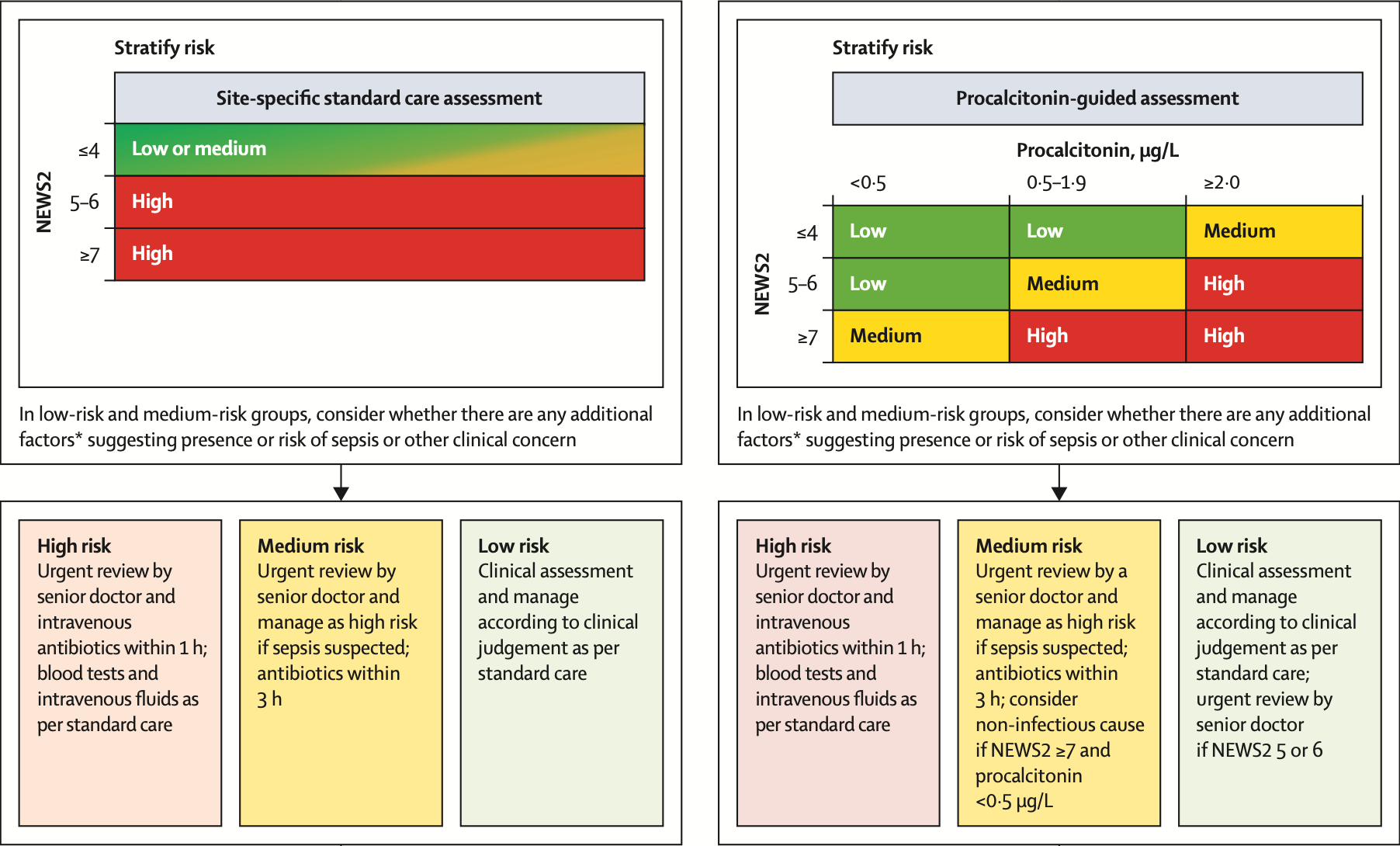
Patients either had “usual [emergency department] care” guided by standard, NEWS2-based sepsis protocols, or had combination NEWS2 + procalcitonin-guided assessment:
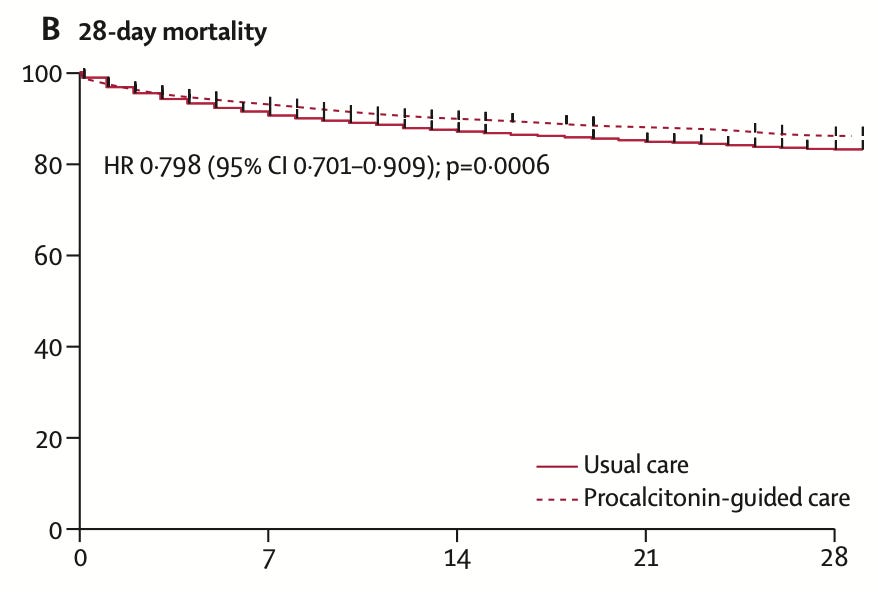
With 7,600 patients randomized, mortality was 13.6% in the procalcitonin-guided cohort and 16.6% with usual care.
The confusing bit – it’s not clear how. Antibiotics were provided to the same proportion of each cohort. Antibiotics within 3 hours were provided to the same proportion of each cohort. No individual subgroup screamed “procalcitonin made all the difference” – and the authors are unable to provide a conclusive explanation for their observed findings.
Even more interesting – only two-thirds of treating clinicians in the procalcitonin arm saw the result, and even fewer agreed with the recommendation arising from the risk score.
The only clue I can see:
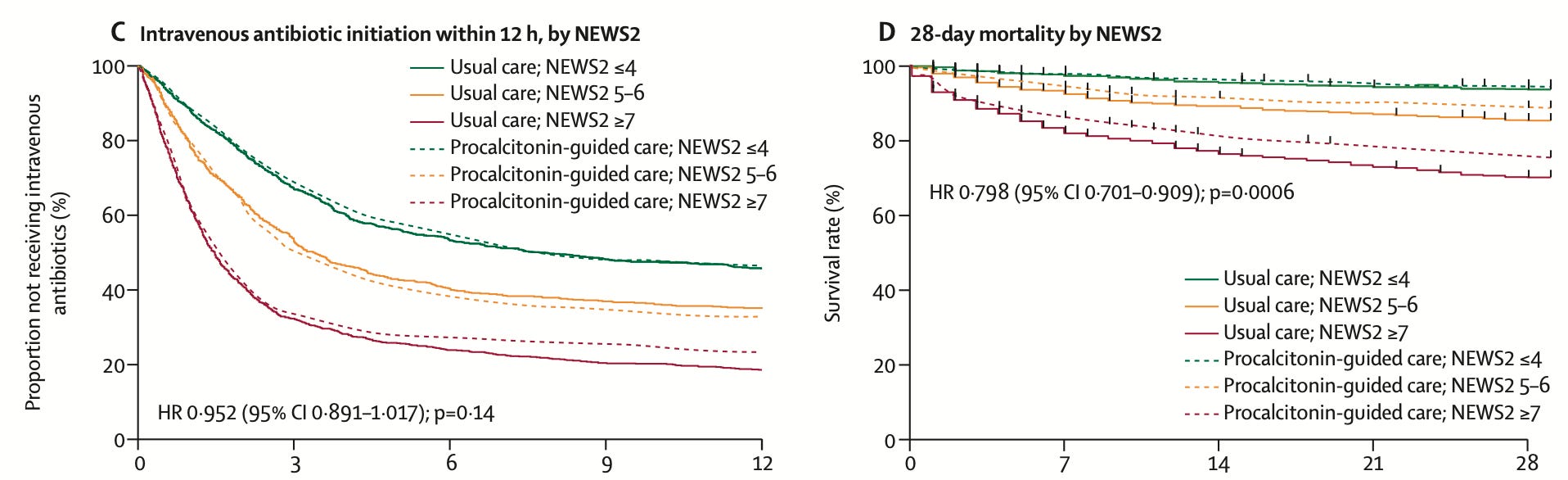
There are slightly different clinician behaviors in the sickest patients, with fewer of them ultimately receiving antibiotics. The only theory I can imagine to explain the results of this trial is the procalcitonin result prevents clinicians from premature closure and anchoring on “sepsis” as a final diagnosis, ensuring alternative diagnoses are explored completely.
These observations are unlikely to reliably generalize outside the settings and models of care similar to those in NHS trusts, but these data still have fascinating implications.