
Sepsis Alerts Are ... Just More Alerts
Yet again with the "not saving lives".
These folks at University of Colorado do a nice job of showing us the world of modern sepsis care, writ pediatric: more alerts, minimal change in clinician behavior, no change in patient-oriented outcomes.
They do this:
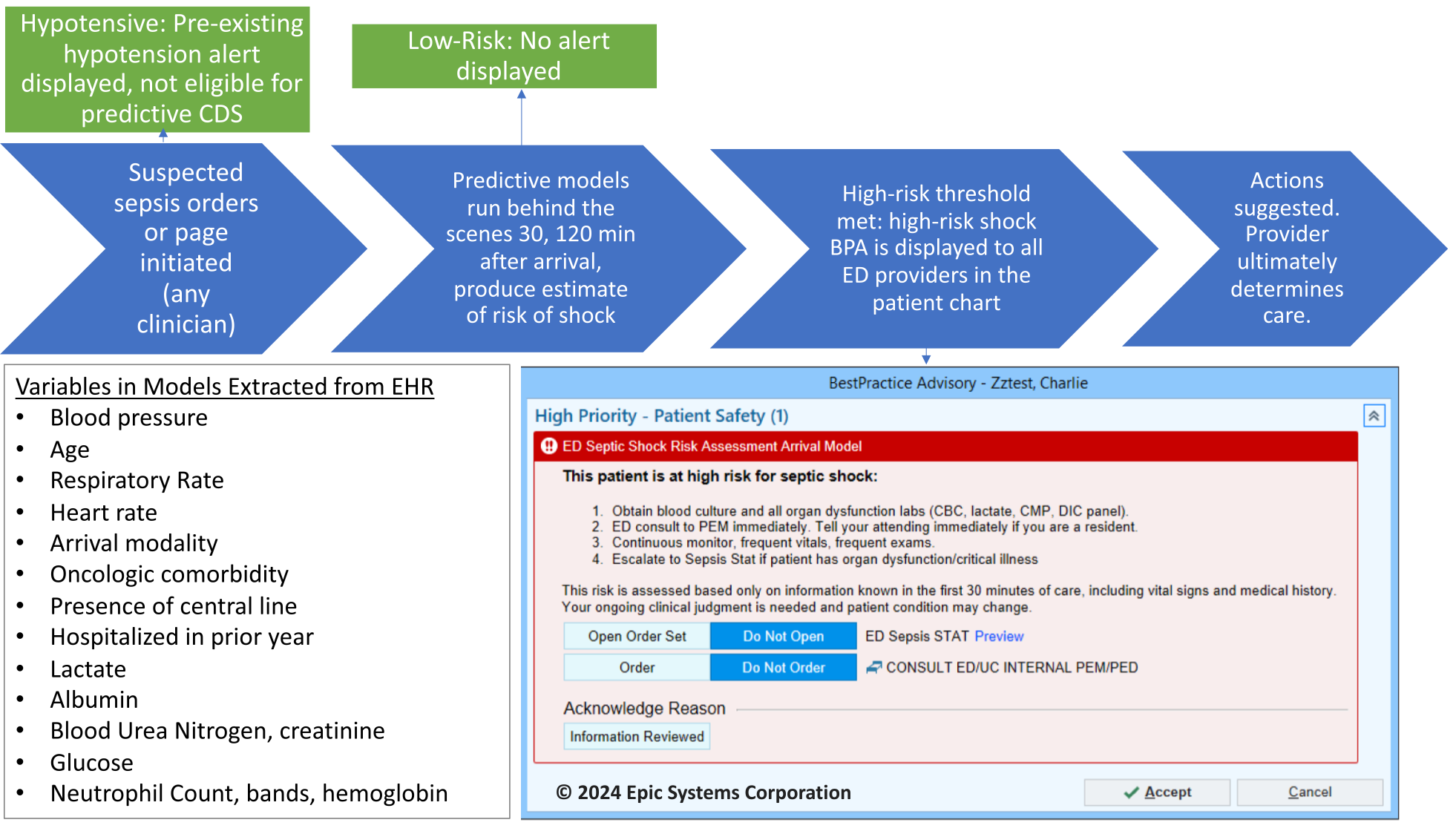
They get this:

The modern clinician does just fine at picking up obvious sepsis without the need for further bothersome alerts, thank you very much.
The only “redeeming” feature notable in this article are some of the subjective responses from clinicians – in that trainees, NPs, and PAs are all somewhat appreciative of the BPA. There are probably roles for additional structure and guardrails to aid less-experienced clinicians, whether BPAs, AI-based tools, or other passive decision-support. However, in the same breath, the clinicians also lamented the BPA burden to which they are already subjected.
The authors go on endorse their BPA plan by noting “all four facilities kept the BPA at the end of the trial” – as if there was truly a choice involved. The hospital sepsis quality improvement program appears to already have had “Sepsis STAT” and “Sepsis Yellow” practices, so the BPA would have needed to be completely intrusive, harmful, or poorly designed to have a chance of being discarded – lack of outcomes data be damned.
Yet another look at the sadly typical response to the supposed sepsis bogeyman. And, with new sepsis legislation coming down the pike, it is likely the sepsis BPA shark has not yet even begun to be jumped.