
Should TNK Always Come Before EVT?
Some do better, some do worse ....
There are many permutations to the “thrombolytics before endovascular intervention” calculation. Should it happen? Should it happen only when there is a long transfer before EVT? Should it happen as an intravascular infusion during EVT? Should it happen with tenecteplase instead of alteplase?
This is BRIDGE-TNK, a typical stroke trial out of China – open-label, approximately 300 patients – testing routine pre-EVT thrombolysis with tenecteplase. As the authors say in their introduction: “Intravenous thrombolysis that precedes endovascular thrombectomy has both the potential benefit of enhancing reperfusion before, during, and after the procedure and the potential risk of increasing intracranial hemorrhage.”
Yep:
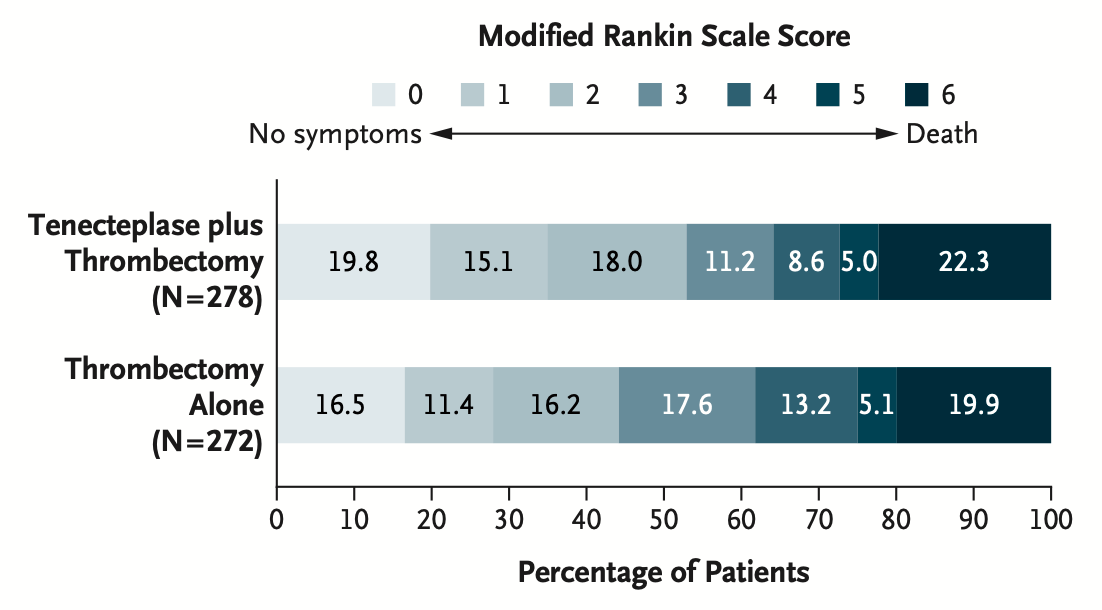
More functional recovery, more death – due, primarily, to an excess of intra- and extracranial hemorrhage.
So, not exactly the entire answer.
Tenecteplase, for what it’s worth, certainly seems to work better than alteplase. However, the reasons it works are complex, and probably related to improved microvascular circulatory effects rather than pre-EVT reperfusion. After all, the difference in reperfusion was only 6% vs. 1%, but the functional outcome difference for mRS 0-2 is 53% vs. 44%. The advantage seems more peri-procedural, rather getting TNK on board on arrival.
The concept seems sound – now, just need to keep working on the safest way to execute.