
The “Rapid Viral Testing" Fallacy
There's no magical reduction in antibiotics as a result of viral testing.
There’s a persistent belief one of the answers to antibiotic overuse and overtesting is ... well, another test. Specifically, one of those rapid microbiology panels capable of canvassing the human petrie dish for a spectrum of viruses and/or bacteria. The theory being, if viruses are detected, the clinicians will place their bets on the result, and the “serious” bacterial infections “requiring” antibiotics are excluded.
Well – they’re half-right.
In this primary care study where clinicians received the results of a BioFire rapid assay, clinicians were indeed less likely to prescribe antibiotics:
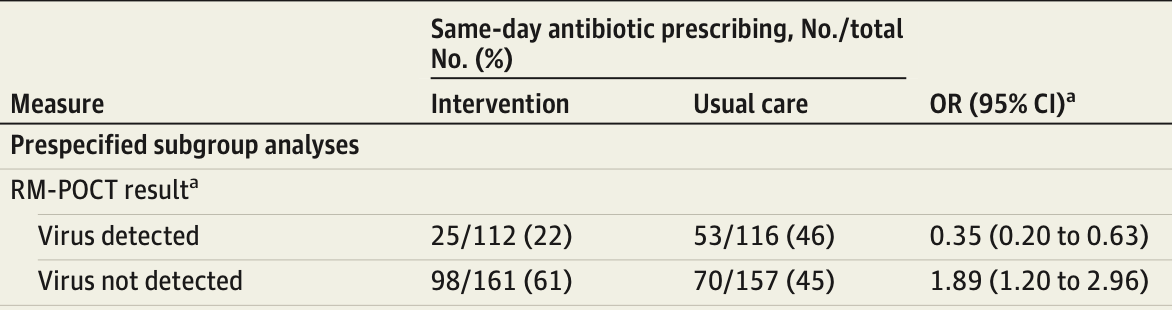
Sadly, however, when no virus was detected – they were *more likely* to prescribe antibiotics. The net overall effect of this viral testing, then, was: zero. Well, except for the added ~$400 cost of the assay.
The information gleaned by the panel provided no improvement in patient-oriented outcomes – regardless of the apparently “better targeted” antibiotic prescribing, both groups improved at the same rate:
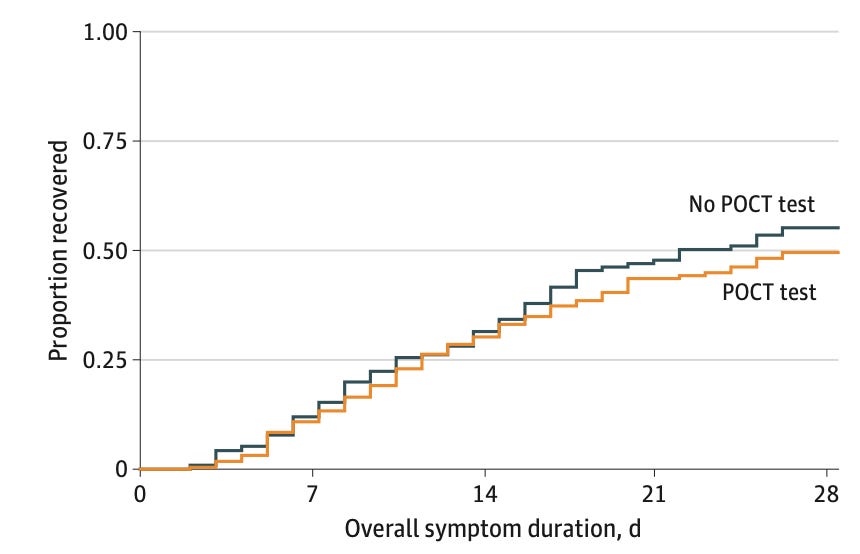
Downstream “second sickening”, repeat prescribing, and other secondary outcomes were likewise no different.
This is further relevant, today, to emergency medicine – where ACEP has put up a draft clinical policy for feedback. This clinical policy, hoping to avoid unnecessary antibiotics and over-investigation in children, is proposing to recommend viral testing for all children under the age of 2 presenting with fever. There is very weak evidence to support this recommendation and, as you can see here, such testing is hardly a panacea for the underlying sociopsychobiomedical issues in the evaluation for infectious diseases.