
Time Is Just A Number
... to steamroll in stroke trials.
Stroke neurology researchers really want you to be able to give thrombolytics for stroke. They really, really, really, really want it. Many of the initial absolute contraindications have been tossed out the window. They’ve tried very hard to justify their practice of giving thrombolytics to minor stroke. And, most famously, they don’t like the current abbreviated time windows.
The latest in their quarter-century pursuit to go beyond the initial 3 hours is the HOPE trial. And, it works:
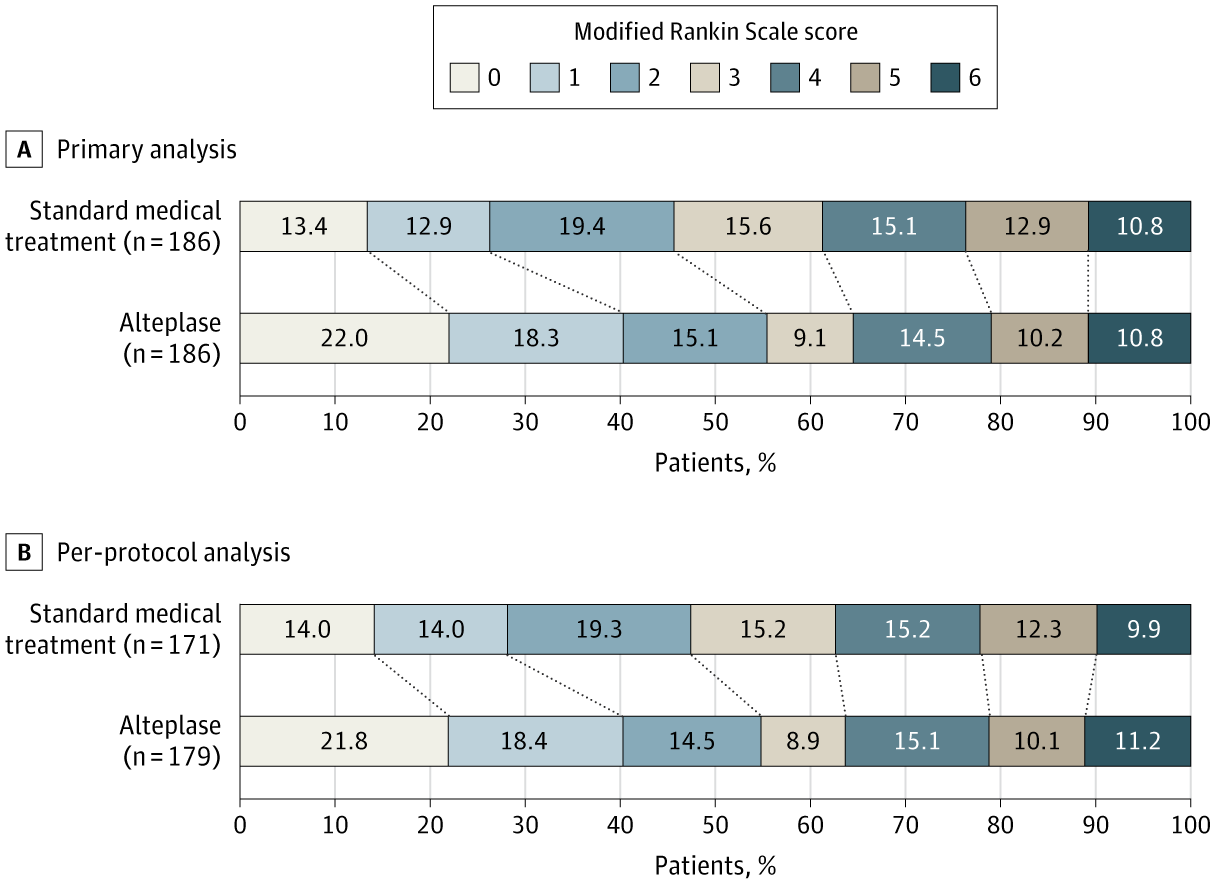
The catch is the same one as all attempts to go beyond 4.5 hours – it requires a favorable mismatch profile on advanced imaging, in this case, CT perfusion scanning. These are also patients who are specifically selected because endovascular therapy was not planned or available – many of these, particularly the 40% with ICA or MCA occlusions, would likely go that route. There was, however, a goodly chunk of M2 occlusions, and the advantage of endovascular treatment for those lesions remains uncertain.
Lastly, there was obviously more intracranial hemorrhage with alteplase – 3.8% vs 0.5%. All-cause mortality is grossly similar, so the ICH doesn’t translate to an excess of harms, but it’s still worth noting in the greater context of this complex triaging decision.