
What Does Our Pursuit of Aortic Dissection Look Like Down Here?
It looks like we're still wandering aimlessly.
In this modern era, it is well-recognized pulmonary embolism is a major vehicle for overdiagnosis. Our increased vigilance has found more PEs, but not improved outcomes. This has prompted much energy to be invested in simply … investigating less.
Aortic dissection does not have the same luxury of benign outcomes if missed, and thus the CT scanner goes brrrrrr. There has been some consideration into using the ADD-RS to reduce over-investigation, but this report from Victoria seems to indicate it is not clearly going to solve our problems with low overall yield:
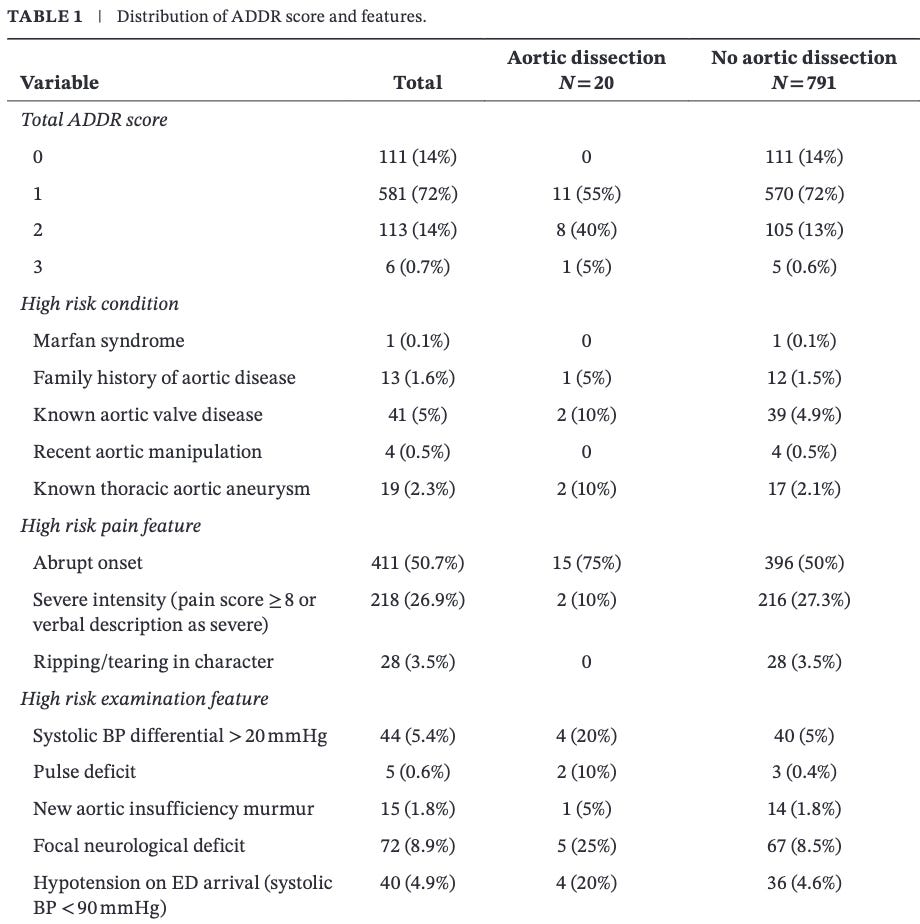
The missing chunk on this data set – ADD-RS is designed to proceed to D-dimer, and these data does not indicate which of these patients incorporated D-dimer in a decision to proceed with angiography. It may the ADD-RS pathway is valid in reducing over-investigation, and there is a whole batch of other patients excluded from angiography based on ADD-RS and D-dimer testing, but these data don’t show us that bit. What it does show us is that it takes 50 CTs, most of which have some “high risk” feature, to find a single aortic dissection.
These data also don’t show us if any important alternative diagnoses were identified on these scans, so it may not be completely hopeless – but I think it goes without saying, whoever can invent A Better D-Dimer can have the next Nobel Prize for Medicine.