
What Reduces Diagnostic Uncertainty in the Emergency Department?
The donut (or ultrasound lasso) of truth.
This is a mildly interesting conceptual study with a grossly unappetizing title – “Entropy removal of clinical features”. Ah, yes, “entropy removal”!
But, underlying this somewhat uninformative title is a substantial analysis of various clinical tests, symptoms/signs, and demographic information and their effects on diagnostic certainty in the emergency department. For example, out of the 405 clinical features derived from 23 citations, here are their Top Five items for enhancing diagnostic certainty in the ED:
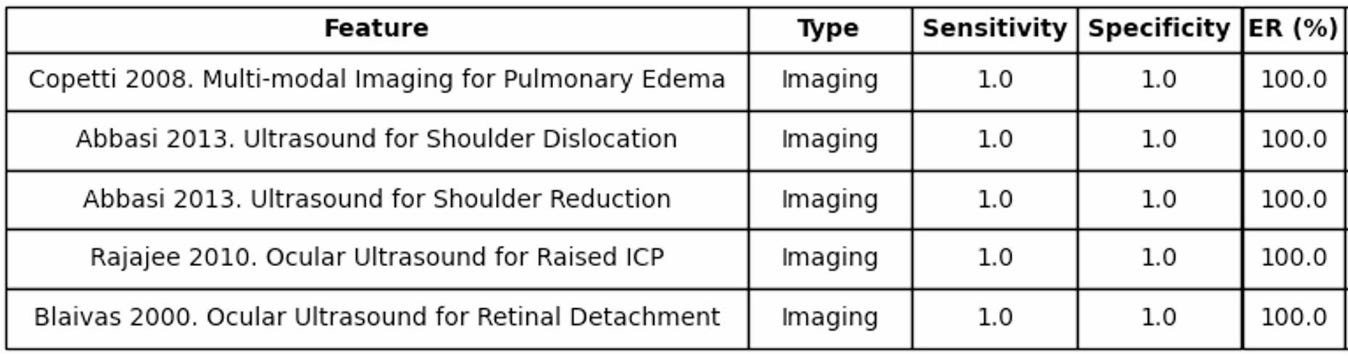
Obviously, to most emergency clinicians, this doesn’t have any face validity as to being a Top Five – the candidate features are obviously limited by the tests and studies included in their reviews – but it does give you an idea the sorts of things that substantially move the needle with good sensitivity and specificity: advanced imaging.
Here are a few more examples, which are likely very familiar to ED physicians working up chest pain in the ED:
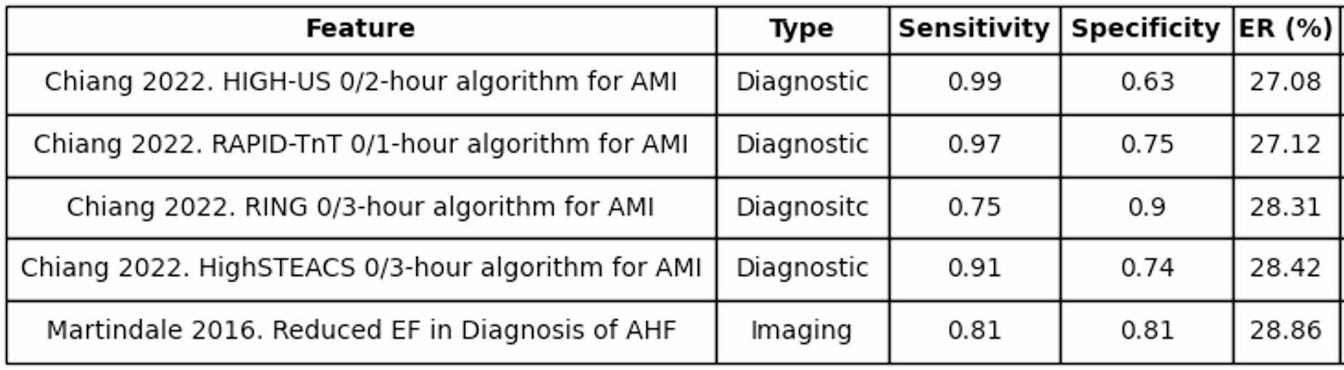
Rapid rule-out and rule-in algorithms for myocardial infarction are heavily relied upon, with sensitivity trumping specificity in most clinical settings.
And, then, as examples of the sorts of things that provide virtually no reduction in diagnostic uncertainty – at least based on the studies they cite:
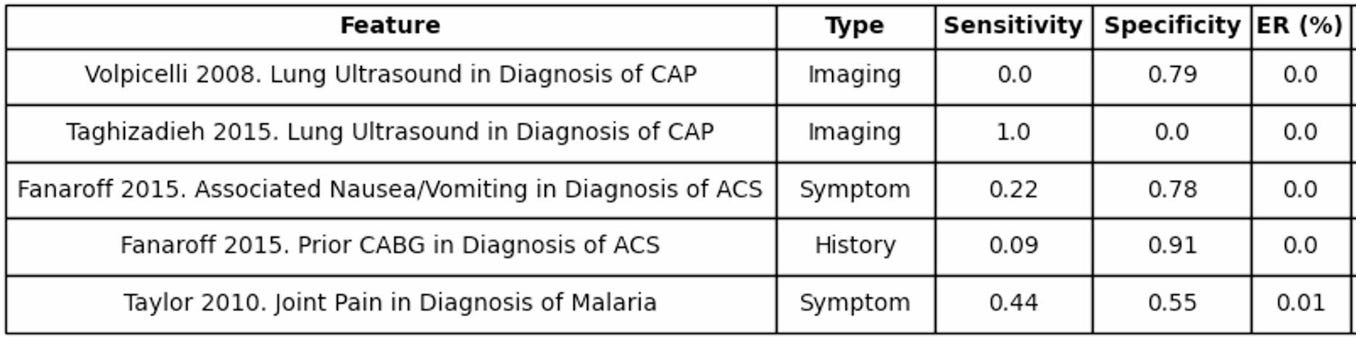
This table is a bit of a good example of where their study breaks down from “usable information” to “fun thought experiment”, demonstrating the limitations of their data source, relying upon citations where lung ultrasound gives either 0% sensitivity or 0% sensitivity, for example.
Regardless, it’s a rather interesting idea – particularly as folks work to refine AI diagnostic engines – to look at where the highest-yield demographics/symptoms/tests contribute to diagnosis in the ED.