
What's This AI Doing Recommending Vasopressin?
It *really* likes vasopressin, which may raise some eyebrows.
Vasopressin holds a funny spot in practice – a guideline-recommended second-line vasopressor with little concrete guidance surrounding the ideal time for its addition to norepinephrine. That said, there is some observational evidence demonstrating advantageous outcomes when initiated earlier in septic shock, at lower doses of norepinephrine, rather than later in disease progression.
That is the starting framing for the OVISS Reinforcement Learning study, which is a complex data dredging of retrospective cohort data to tease out any useful insights in how to deploy vasopressin.
Effectively, the model combed through the septic shock data from UCSF hospitals looking at the clinical features of patients who received vasopressin. Within these data, the model shook out the features associated with timing of vasopressin administration and favorable outcomes as compared with the other, most similar, patients in the data set. A model was then arrived at approximating the ideal clinical use for vasopressin, which was then validated on several external data sets.
An illustrative example of how practice might change is in this figure:
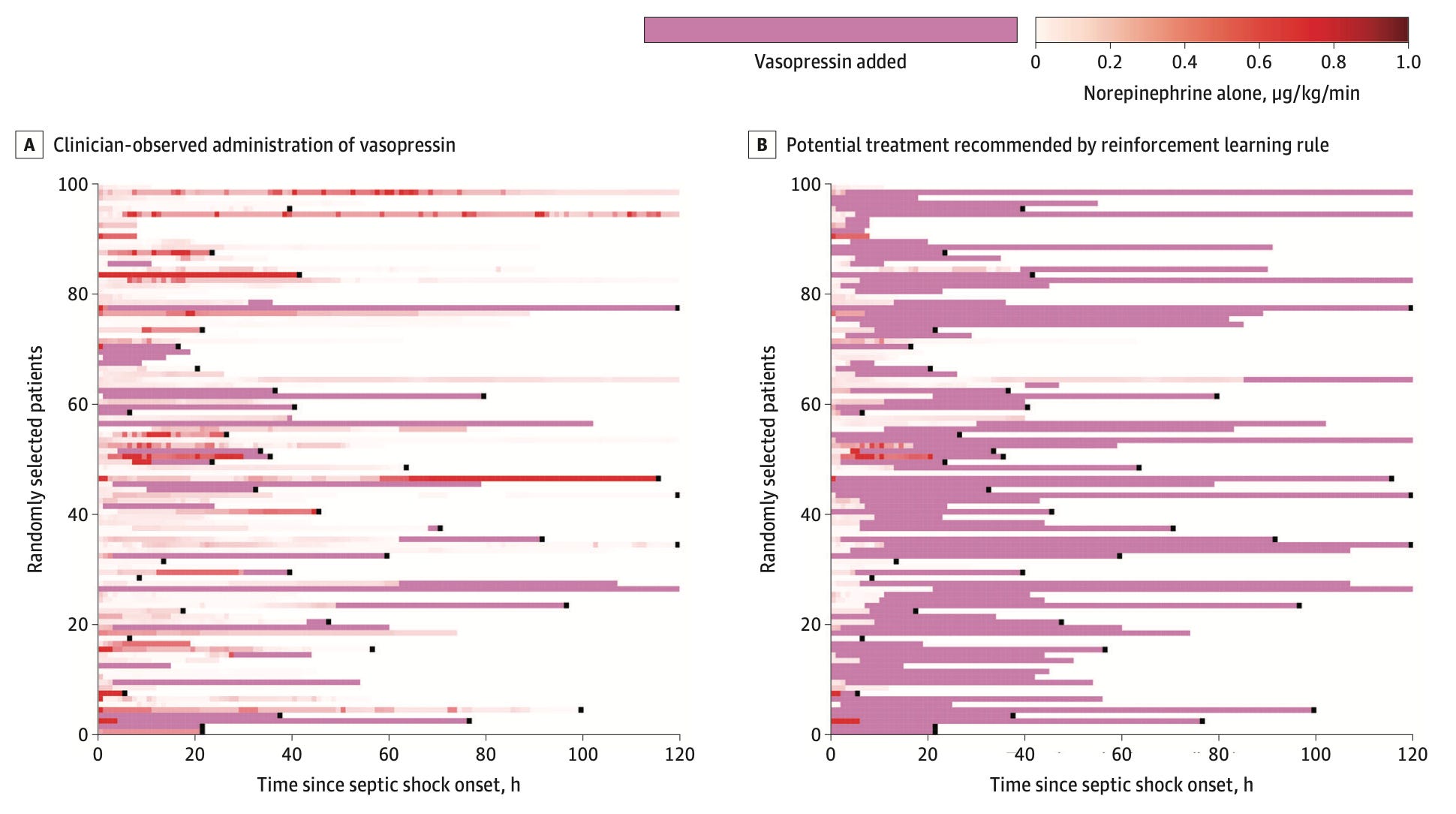
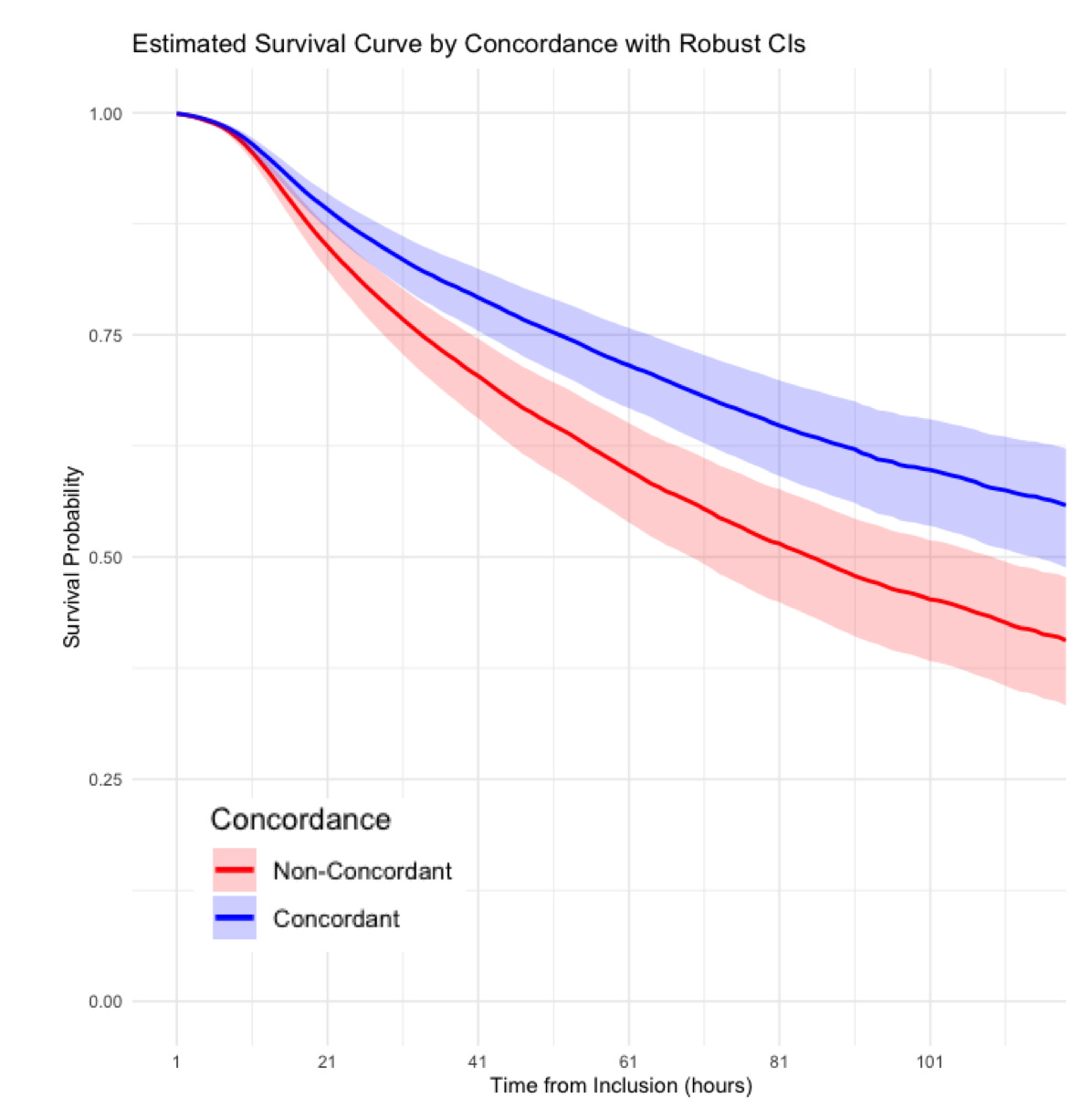
And, if clinicians behaved as the model recommended – initiating vasopressin in nearly 90% of patients instead of 30%, and at much earlier time points – predicted mortality would look like this:
Essentially, the model suggests a far more aggressive use of vasopressin than observed in typical practice – perhaps consistent with some of the observational data out there.
Nice study – now, go validate it prospectively!