
"Whole Blood" Versus "Pieces of Blood"
It didn't generally matter in this trial.
Transfusion trends in traumatic hemorrhage have changed over the course of my career. Originally, blood was simply packed red cells. Then it became important to add plasma. Then the ratio of plasma became important. Now, “whole blood” is in vogue.
But, this trial involving prehospital transfusion following major trauma found no difference between whole blood and balanced blood components for their primary outcome:
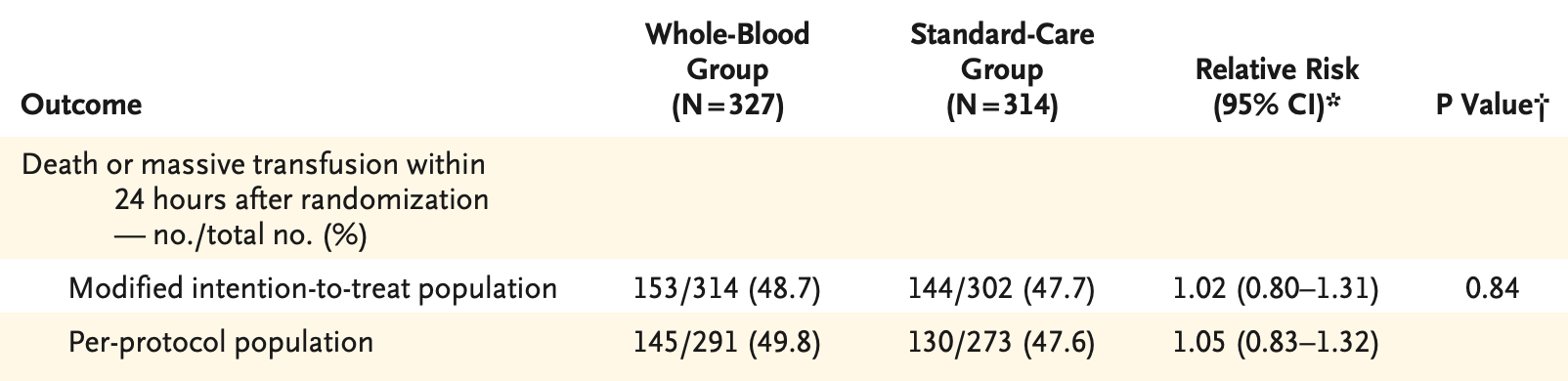
“But what’s the breakdown of the massive transfusion component” you ask, and thus some secondary outcomes:
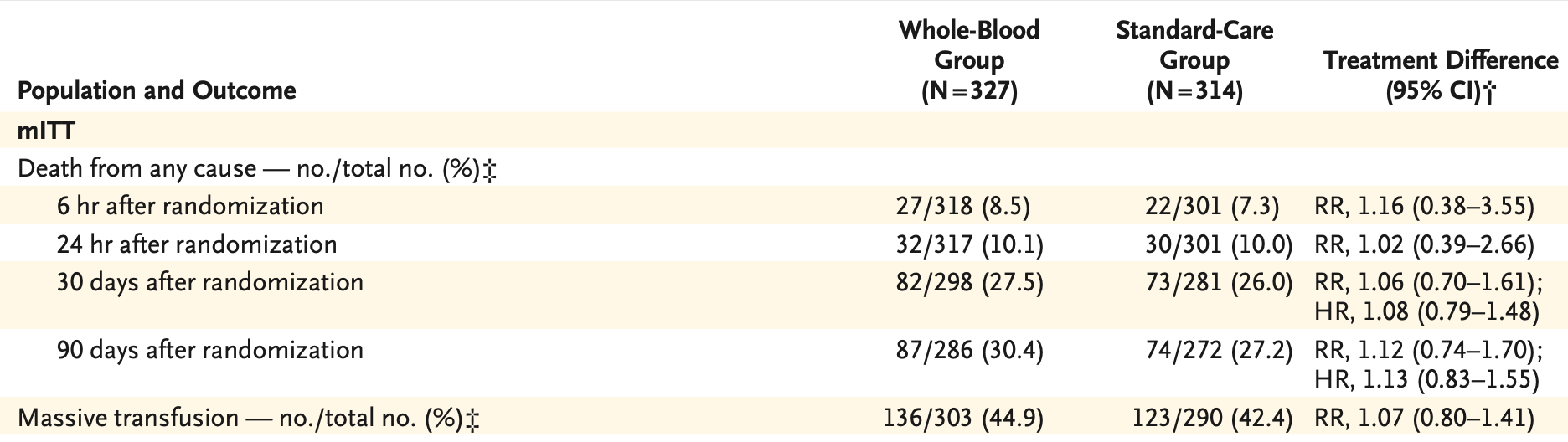
Prothrombin times were longer in the whole blood component group on arrival, but it is doubtful this translated into any meaningful differences in primary, secondary, or safety outcomes.
It’s possible limitations in the trial did not enroll the proper cohort from which to detect an advantage to whole blood – but it’s probably more likely there simply isn’t one.
This is an excellent summary. One factor that has been omitted from existing studies and that may be critical is the ABO blood group of the recipient, and the number of ABO mismatched blood transfusions administered. Another is that there are data from the 1980s/90s that demonstrate that whole blood may be more harmful to patients than red cells alone, particularly if not leukoreduced. Br J Surg. 1992 Jun;79(6):513-6. doi: 10.1002/bjs.1800790613. PMID: 1611441. Ann Surg. 1988 Apr;207(4):410-5. doi: 10.1097/00000658-198804000-00007. PMID: 3355265; PMCID: PMC1493418. Whole blood has white cell debris, platelets, microparticles, HLA antigens, NETs present in much greater concentrations than in red cells. These are likely mediators of the dose dependent increase in thrombosis, nosocomial infection, organ injury, inflammation and mortality seen in most transfusion studies, including randomized trials.
ABO blood group matters because group O patients bleed more, perhaps contributing to early hemorrhagic death in trauma patients. Group A, B and AB patients thrombose more, perhaps contributing to later death due to multi-organ failure in these patients. Group AB patients are more likely to receive many ABO mismatched transfusions, perhaps leading to increased low level hemolysis and endothelial injury due, in particular to anti-A. So examining the patient's ABO type and receipt of ABO mismatched transfusions should be a part of every such study in the future. Group O whole blood has the potential advantage of being ABO identical with 45% of recipients. Current blood bank practices lead to 100% of trauma patients receiving ABO mismatched transfusions when components are given (usually O red cells, any old ABO platelets, usually A, and AB or A plasma, and any old cryoprecipitate). This is due to erroneous dogmas that have no evidence. So it may be that low titer group O whole blood, if superior, is because it contains the least incompatible ABO antigen and antibody. Let's hope so.
We have summarized these issues recently in Whole Blood versus Components for Transfusion in Trauma and Life-Threatening Hemorrhage-Unresolved Issues. Anesth Analg. 2026 Jan 13. doi: 10.1213/ANE.0000000000007923. Epub ahead of print. PMID: 41529673.
I would also point out that presenting 24 hour and 30 day mortality is not the optimal way of expressing survival data for published studies. Have no idea why the statisticians involved in these studies sanctioned such potentially misleading presentation of the data. More appropriate is 24 hour survival coupled with either hospital discharge alive or long term survival by Kaplan-Meier and Cox regression analysis. From a patient standpoint and statistical precision standpoint, these are more meaningful. If one dies at 31 days or 41 days, etc., it's just as unfortunate, particular from the patient's perspective :).
In summary, it may well be that group O whole blood is superior to component therapy because it is less harmful from an ABO antigen-antibody interaction perspective rather than being more efficacious. In other words, current blood transfusion service practices for component therapy are so harmful to patients that group O whole blood is less harmful. From a hemostasis standpoint there is little reason to think that whole blood is more effective than separated red cells, plasma and platelets, for example. Indeed part of the issue with our current practices may be that many patients who just need crystalloid and red cells are receiving plasma and platelets that are not only not necessary but harmful through their pro-thrombotic, inflammatory and immunomodulatory effects.