
Does It Matter: Slow Dilution or Fast Dilution?
For hypernatremia, it might not.
I’ve seen this study floating around the socials because, like many dogmatic things, rates of correction in hyper- and hyponatremia are a bit like oral histories of the world being passed down from wise sage to wise sage. Many of these stories turn out to have kernels of truth, while some are mostly legend.
The study in question tests the legend of slow vs. fast correction for patients with severe hypernatremia, distilling down the MIMIC-IV 3.0 cohort for a propensity-matched comparison:
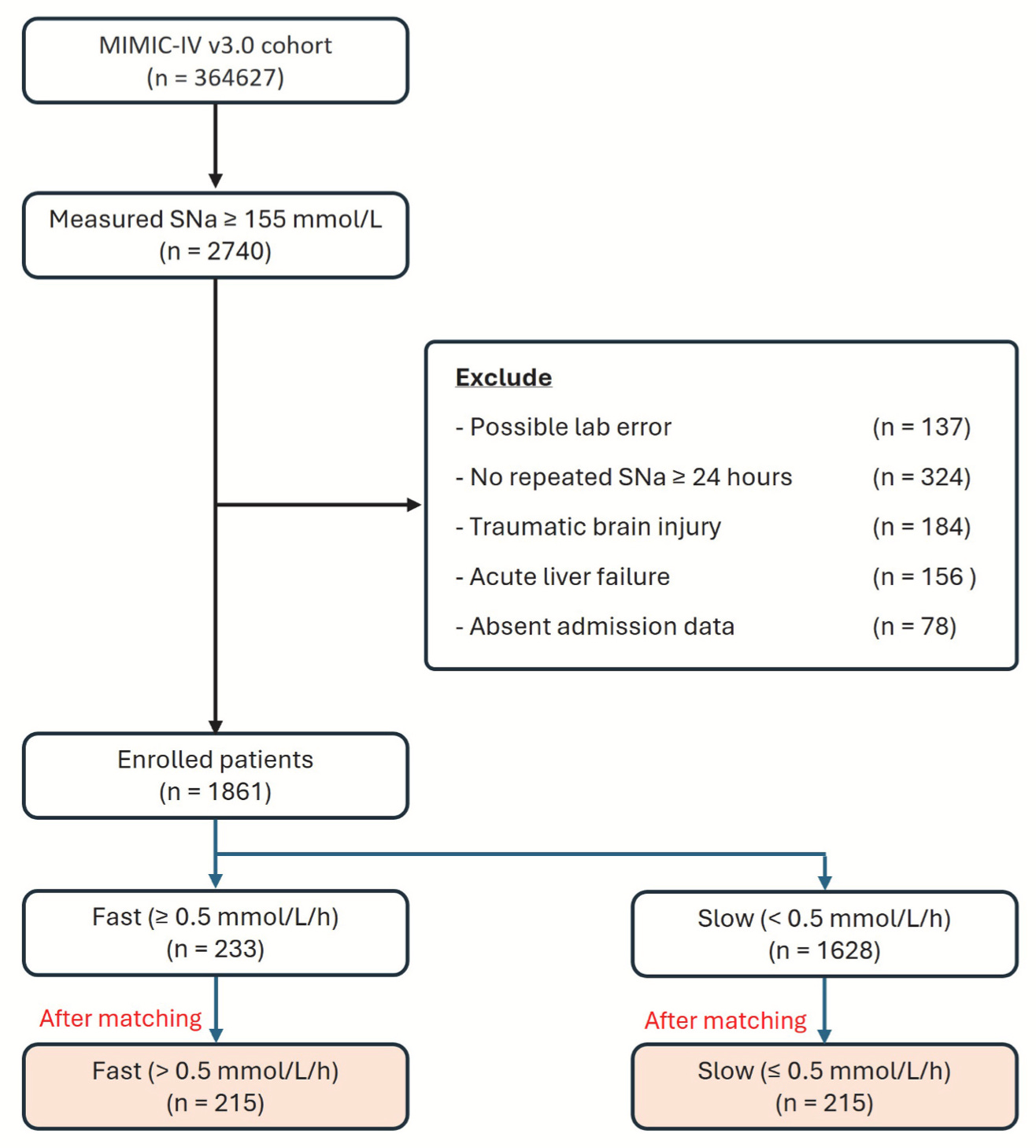
The winner: the fast correction cohort, with a 30-day mortality of 10.3% versus 22.4% for the slow.
The folks who received rapid correction are Not Like those who received slow – there is propensity matching, yes, but that only joins up a handful of baseline characteristics. It does not capture a full picture of the clinical problem precipitating the hypernatremia, the entirety of the acute treatment, and the clinical context in which the fast correction could tolerate a positive fluid balance of 2.5L in the first 24 hours, as compared to the 1L for the slow correction.
Regardless, these data provide reasonable scaffolding to question the need for slow correction – and could inform practice in situations where a clinical need for fluid resuscitation takes priority.